Yesterday, the UK Health Security Agency (UKHSA) published a news story urging timely whooping cough vaccination in pregnancy and in childhood to protect vulnerable young infants from serious disease:
- Pregnant women are offered a whooping cough vaccine in every pregnancy, ideally between 20 and 32 weeks – protecting their baby from birth in the first months of their life when they are most vulnerable and before they can receive their own vaccines.
- All babies are given three doses of the 6-in-1 vaccine at 8, 12 and 16 weeks of age to protect against whooping cough and other serious diseases.
New data published yesterday by UKHSA shows cases of whooping cough continue to increase with 2,591 cases confirmed in May. This follows 555 cases in January 2024, 920 in February, 1,427 in March and 2,106 in April – bringing the total number of cases from January to May 2024 to 7,599.
Sadly, there have been 9 infant deaths since the current outbreak began in November last year (one in December 2023 and 8 between January to end May 2024). Young babies are at highest risk of severe complications and death from whooping cough. Evidence from England shows that vaccination at the right time in pregnancy is highly effective, giving 92% protection against infant death.
From January to May 2024, while most cases (53.4%, 4,057) were in those aged 15 years or older who usually get a mild illness, high numbers (262) continue to be reported in babies under 3 months of age who are at greatest risk from the infection.
Whooping cough cases have been rising across England, as well as in many other countries, since December 2023 due to a combination of factors. Whooping cough is a cyclical disease that peaks every 3 to 5 years. The last cyclical increase occurred in 2016. However, in common with other diseases, cases fell to very low numbers during the pandemic due to restrictions and public behaviours. A peak year is overdue and the impact of the pandemic also means there is reduced immunity in the population.
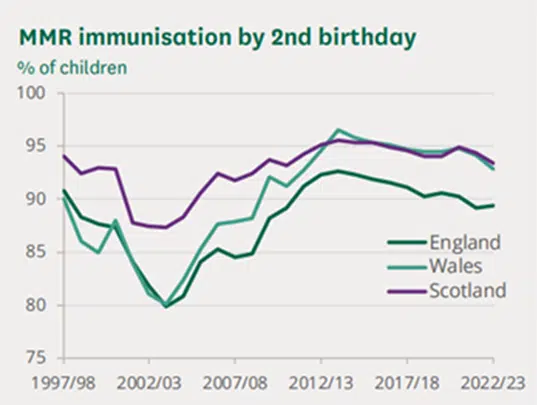
The latest uptake data for the vaccination offered to pregnant women to protect newborn infants against whooping cough continues to decline – with coverage in March 2024 at 58.9% compared to the peak coverage (72.6%) in March 2017.
Timely vaccination in pregnancy and in childhood are both important to protect vulnerable young infants from serious disease. All babies are given three doses of the 6-in-1 jab at 8, 12 and 16 weeks of age to protect against whooping cough and other serious diseases such as diphtheria and polio, with a pre-school booster offered at 3 years 4 months.
Whooping cough, clinically known as pertussis, is a bacterial infection which affects the lungs. The first signs of infection are similar to a cold, such as a runny nose and sore throat, but after about a week, the infection can develop into coughing bouts that last for a few minutes and are typically worse at night. Young babies may also make a distinctive ‘whoop’ or have difficulty breathing after a bout of coughing, though not all babies make this noise which means whooping cough can be hard to recognise.
If anyone in your family is diagnosed with whooping cough, it’s important they stay at home and do not go into work, school or nursery until 48 hours after starting antibiotics, or 2 weeks after symptoms start if they have not had antibiotics. This helps to prevent the spread of infection, especially to vulnerable groups, including infants. However, vaccination remains the best protection for babies and children.
UKHSA Blog
Alongside the updated data, UKHSA also published a powerful new blog post, “Whooping cough: my daughter spent the third week of life in an induced coma”. In this blog post, Jenny, from Hampshire, shares the story of her daughter Layla and her struggle with whooping cough at 3-weeks-old.
Health visitors’ role to promote uptake of the pertussis vaccine
UKHSA is calling for frontline clinicians to promote uptake of the pertussis vaccine. Pregnant women can have a pertussis-containing vaccination between 20 and 32 weeks’ gestation – they should also be vaccinated with every pregnancy.
Health visitors have a vital role to play in discussing vaccinations with parents and caregivers and promoting vaccine uptake. As a universal service, they visit every family, building trust through regular visits, often in the family’s home. Resources are available for health visitors and their team members to support communication around vaccines with pregnant women.