The annual publication of the MBRRACE-UK ‘Saving Lives, Improving Mothers’ Care’ report is always sobering. It prompts reflection on the circumstances that contributed to the death of women in the perinatal period, leaving babies without mothers and families coping with devastating consequences. The findings of the twelfth report were shared at the MBRRACE-UK Virtual Conference on 11 September framed by the understanding that, behind the statistics, were real women.
The 2025 MBRRACE-UK report looks at the care of 643 women who died during or up to one year after pregnancy in the UK and Ireland. Of these women, 583 (91%) faced multiple interrelated challenges including social service involvement, domestic abuse and deprivation.
Of note:
- In 2021-23, 257 women died during or up to six weeks after pregnancy among 2,004,184 women giving birth in the UK. This represents a maternal death rate of 12.82 women per 100,000 women giving birth.
- This was a statistically non-significant decrease in the overall maternal death rate in the UK in 2021-23 compared to 2020-22, but still higher than the period 2018-20.
- Thrombosis and thromboembolism remained the leading cause of maternal death in 2021-23 followed by cardiac disease and COVID-19.
- The highest rate of death occurred between 6 weeks to 1 year postnatally (classed as late maternal deaths). The rate of late maternal deaths has continued to increase and was significantly higher in 2021-23 than in 2018-20.
- Suicide was the leading cause of late maternal death, followed by deaths due to substance use.
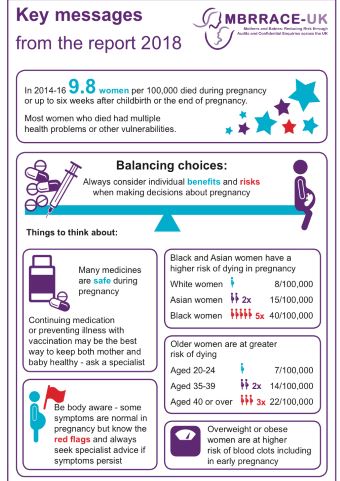
- Significant inequalities in maternal mortality rates persist among women living in the most deprived areas and women from Black and Asian ethnic backgrounds.
This year’s confidential enquiries into maternal deaths identified lessons learned from the care of women who died from hypertensive disorders of pregnancy, cardiac disease, mental health-related causes, homicide and accidents.
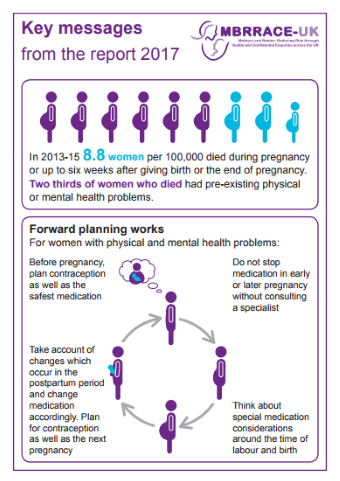
Assessors identified many common themes across these topics including the importance of pre-pregnancy counselling and getting women ‘ready for pregnancy’. This includes counselling women about their risk factors, optimising medications and discussing risk-reduction strategies such as weight loss or smoking cessation. Assessors emphasised that recognition of risk factors must also include social or mental health complexities, which should be considered alongside physical health.
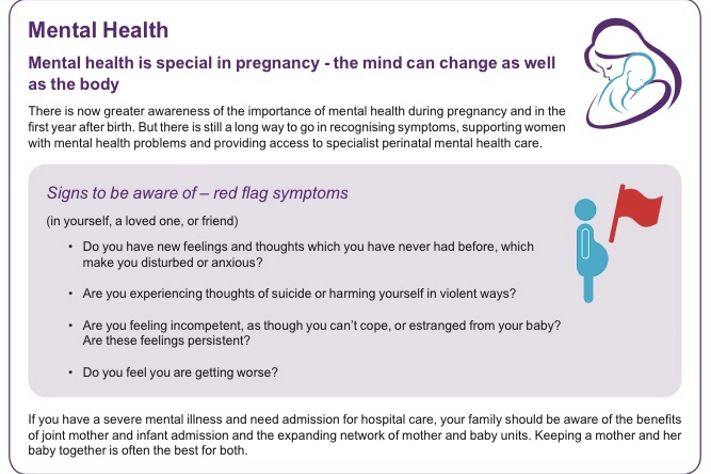
** 34% of late maternal deaths were due to mental health-related conditions **
The confidential enquiry into the care of women who died from mental health-related causes once again highlights the significant impact that the loss of a child, either through early pregnancy loss, bereavement or custody loss, can have on mental health. These women may require additional support during and after pregnancy, regardless of how their pregnancy ends.
It remains imperative that ‘red flag’ signs and symptoms are thoroughly investigated. It is important to recognise decline and conduct an urgent assessment if women present with new symptoms, thoughts or acts of violent self-harm, or expressions of incompetency as a mother or estrangement from the infant.
Alison Morton, CEO of the Institute of Health Visiting, said:
“The publication of this annual report is always time to take stock. Sadly, too many women are dying from conditions that could have been prevented through better care. And we know that ongoing cuts to health visiting services are only widening the gaps in care. In particular, the findings on late maternal deaths provide a stark warning on the current state of postnatal care – and are highly relevant to health visiting and healthcare policymakers.
When adequately resourced, health visitors provide vital postnatal care and opportunities for early identification of risk during this period of heightened vulnerability – as the only service that proactively and systematically reaches all women during this time. This role needs to be maximised!
At the iHV we are continuing to call for increased and sustained investment in the profession. Health visiting is a safety-critical workforce during the perinatal period, particularly for those families who experience complex, multiple disadvantage. The MBRRACE report highlights that effective communication and interagency working remain essential to recognise complexities, coordinate care and prevent future maternal deaths. We are committed to ensuring that health visitors continue to play a key role in this.”
New national recommendations for the care of women with medical and social challenges include:
- Urgent referral pathways: setting up an urgent referral pathway to triage high-risk women for senior or specialist review in early pregnancy
- Information sharing: ensuring codes for domestic abuse in women’s records are used and information is shared appropriately in the event of safeguarding concerns
- Discharge summaries: including a summary box of actions concerning conditions that require postnatal management