12th August 2024
We are delighted to share this Voices blog by Dr Ruth Naughton-Doe, NIHR Postdoctoral Research Fellow at the University of York, who reviews her recent research and findings on preventing perinatal loneliness.

Dr Ruth Naughton-Doe, NIHR Postdoctoral Research Fellow, University of York
My journey exploring how to prevent perinatal loneliness began when I was diagnosed with postnatal depression in summer of 2021. I felt overwhelmed and lonely, and despite being a passionate advocate of ending such stigma, I also felt ashamed.
Yet, I was fortunate. I soon felt better thanks to excellent support from mental health services and my family. I also joined a local parent and baby walking group, and meeting other parents with similar experiences helped me feel less alone. Motivated to understand how we can better support parents to avoid experiences like mine, I later secured research funding to explore how to prevent perinatal loneliness. Supported by my supervisors (Professor Webber, Dr Tierney and Professor Wittkowski) and two advisory groups of diverse professionals and people with lived experience, the research began in October 2022.
What is perinatal loneliness and why does it matter?
Perinatal loneliness is the loneliness experienced by parents and prospective parents during pregnancy and up to two years post-birth. This includes partners and those who have children via adoption, surrogacy, and other means. Any parents can feel lonely, but parents are more at risk if they are from disadvantaged communities, or feel excluded due to their age, gender, ethnicity, religion, sexuality, or due to a health issue or disability1. There is evidence to suggest that loneliness can cause perinatal mental illness or make existing problems worse2. Addressing loneliness may therefore prevent or stop the worsening of perinatal mental illness. Through this study, I aimed to find out what interventions and societal changes might be effective.
Research approach
The project began with a literature review to identify the types of interventions, services and activities that had been described and/or evaluated. I then led a study to hear diverse parents’ and practitioner perspectives. Forty-eight parents and nineteen professionals participated, including fathers, LGBTQ+ families, Muslim parents, neurodiverse parents, and parents with poor mental health.
Types of loneliness
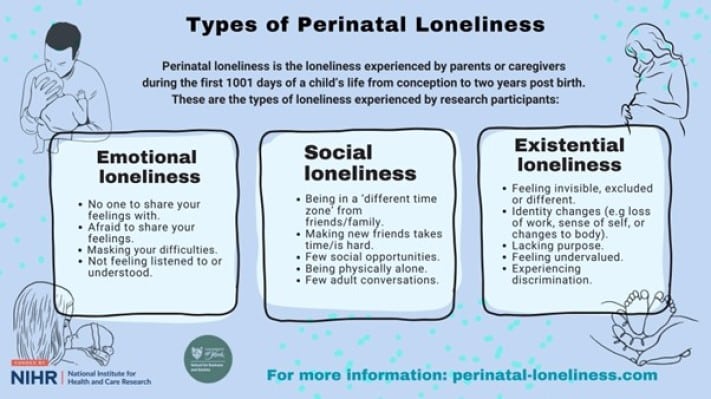
Parents shared stories of three types of loneliness. Social loneliness was present when parents lacked a fulfilling social network, and emotional loneliness occurred when they had too few people to confide in. Parents felt existential loneliness if they felt disconnected from their former selves, undervalued, or felt excluded and/or unwelcome. Whilst transient feelings of loneliness that occur during a specific time-limited period can sometimes be dismissed as less serious than chronic loneliness, the first 1001 days is such an important time for child development, it is vital that we support parents better.
Why did parents feel lonely?
Parents reported that they were unprepared for the challenges of parenthood, worried whether they were caring for their baby correctly, and did not know who to ask for help or who to trust. Many parents felt guilty and ashamed for not living up to their idealised image of a good parent, and hid their feelings from others, including from professionals.
Caring for a young baby meant parents had little time for themselves or to see others, which contributed to changed relationships with partner, friends and family. Many parents felt that public transport and public spaces did not feel family friendly or inclusive to their needs. Parents felt parental leave was too short and left one parent alone to care for their baby, whilst the other went to work and missed out on bonding with their child.
Most parents were not satisfied with statutory support from health and care services. Since 2010, there has been a more than 40% reduction in health visitor numbers3, and a 45% reduction in early intervention services, such as Sure Start4. Professionals emphasised they often had to prioritise crises rather than delivering the preventive, holistic, personalised and inclusive support they aimed for.
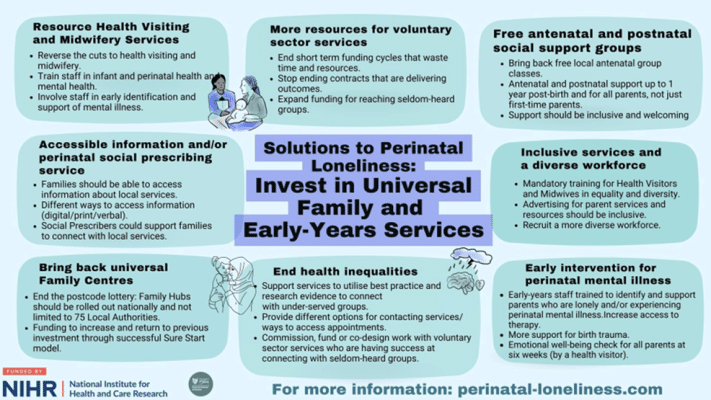
What changes do parents want?
- More support from statutory services, including Health Visiting services, which have been shown to be effective at reducing perinatal loneliness. More funding for these services is essential so they have the resources to identify and support parents who feel lonely.
- Paid leave for both parents. More time would allow both parents to bond and care for their child whilst maintaining their social networks and self-care.
- Services to be inclusive for people of all ages, genders, ethnicities, religions, sexualities, health and disability statuses.
- Free, inclusive and fun activities for parents that are specifically aimed at building their social connections and improving wellbeing.
What can health visitors do?
- Routinely include the assessment and identification of loneliness and perinatal mental health difficulties in health visiting practice.
- Be aware of the different types of loneliness. A parent may appear to have a strong support network but could still be feeling lonely.
- Build on parents’ strengths and encourage them to explore solutions that may work for them in order to look after their own wellbeing.
- Include fathers and non-birthing parents in all support. Parents wanted to feel equally involved, valued and supported.
- Attend training in equality and diversity, and utilise inclusive language.
For more information, please see the full report.
This project was funded by the NIHR Three Schools Mental Health Programme (Fellowship Award Number: MH051). The views expressed in this report are those of the author and not necessarily those of the NIHR or the Department of Health and Social Care. July 2024
Dr Ruth Naughton-Doe, NIHR Postdoctoral Research Fellow, University of York
www.perinatal-loneliness.com
@pn_loneliness
[email protected]
@ruthndwrites
To learn more about supporting family wellbeing, join us for our iHV Perinatal and Infant Mental Health In Focus Conference: Dismantling the Barriers – collaborative approaches to perinatal mental health care. This half-day virtual conference is taking place on 19 September 2024. Book your place here!
To learn more about the Perinatal Loneliness Project, join Dr Ruth Naughton-Doe for the Perinatal Loneliness online conference, taking place on 18 September 2024.
References
- Taylor BL, Howard LM, Jackson K, Johnson S, Mantovani N, Nath S, Sokolova AY, Sweeney A. Mums Alone: Exploring the Role of Isolation and Loneliness in the Narratives of Women Diagnosed with Perinatal Depression. J Clin Med. 2021 May 24;10(11):2271. doi: 3390/jcm10112271.
- Adlington K, Vasquez C, Pearce E, Wilson CA, Nowland R, Taylor BL, Spring S, Johnson S. ‘Just snap out of it’ – the experience of loneliness in women with perinatal depression: a Meta-synthesis of qualitative studies. BMC Psychiatry. 2023 Feb 28;23(1):110. doi: 1186/s12888-023-04532-2.
- Institute of Health Visiting. State of Health Visiting: UK survey report. London: Institute of Health Visiting 2024
- Franklin J, Larkham J, Mansmoor M. The well-worn path. Children’s services spending in 2010-11 to 2021-22. London: Pro Bono Economics and Action for Children 2023.




