28th April 2025
How can we improve peer and community breastfeeding support so that it meets the needs of all mothers?
This iHV Voices blog is by Dr Rabeea’h Waseem Aslam and Joelle Kirby – both are systematic reviewers in the National Institute of Health and Care Research (NIHR) Public Health Reviews Team, which includes experts from the Universities of Exeter, Cardiff and Birmingham.
The blog gives an overview of the findings and recommendations from two NIHR-funded research reviews – ‘Peer support and community interventions targeting breastfeeding in the UK: Systematic review of qualitative evidence to identify inequities in participants’ experiences’ and ‘Equity-focused peer support and community interventions for breastfeeding in high-income countries: Systematic review and intervention component analysis’.

Dr Rabeea’h Waseem Aslam
The UK is known for having some of the lowest breastfeeding rates in the world. For some women, this is because they have decided it is not the right choice for them and their family. However, for many others, they want to breastfeed but have stopped because they find the experience difficult and don’t receive the right type of support.
Programmes delivered in a woman’s home or local area have been developed to try and help women navigate the challenges they encounter. These include peer support, where trained women with similar social or cultural backgrounds help mothers by offering advice and encouragement. There is also community support, given by non-hospital-based healthcare professionals (e.g. community health visitors) and non-healthcare professionals.
But some communities of women don’t get to access to these programmes or, when they do, they may have negative experiences. This can lead to inequalities in breastfeeding rates.
We looked at research evidence to help understand how peer and community support services could be delivered to make sure that all women have a positive experience and are encouraged and supported to breastfeed if they want to.
We conducted two reviews of previous research. One to draw together qualitative evidence from the UK to understand how the characteristics of mothers shaped their experiences of peer and community support. And another to look at evaluations of peer and community support in higher-income countries to understand what activities are currently delivered to and if they prevent inequities in breastfeeding rates.
What we found
There were different experiences of peer and community programmes, which may lead to inequities in breastfeeding rates. For example:
- A lack of clear information on who can access them. This may have a disproportionate effect on the likelihood of women from black and minority communities engaging.
- Limited options to access support due to it being delivered at inconvenient times or in inaccessible locations. For example, women reliant on public transport can find it difficult to get to venues and they may find the cost prohibitive.
- Inadequate consideration of mothers’ social and cultural background, and how this might shape their needs. For example, mothers from a range of cultural backgrounds may feel uncomfortable breastfeeding in front of others, both outside and within the home (especially if living with extended family).
- Lack of consideration of different physical characteristics, such as body type and disability. For example, breastfeeding materials rarely present visuals of mothers with darker skin tones or larger bodies.
- Structural barriers such as unsupportive workplace breastfeeding policies, lack of support from family members, and wider social stigma. For example, formula feeding is often seen as the norm in some communities.
How to ensure peer and community support meets the needs of all mothers?
We identified five principles (see Figure 1) that might help to make peer and community breastfeeding support more equitable:
- Support should come from people with similar backgrounds or experiences, such as other mothers who have breastfed. This can help foster trust and make it more likely that mothers will be encouraged to take part.
- Eligibility criteria and access routes for programmes need to be promoted throughout the breastfeeding journey so that mothers are aware of the support available to them. There is also a need to provide women with flexibility in how and when they can receive support.
- Messaging and provision of services should be tailored to meet different individual and community needs. This should be done without causing stigma or reinforcing stereotypes. For example, being seen as non-judgemental about feeding choices can help mothers who do not exclusively breastfeed feel more welcome.
- Transitions between programmes, for example moving from one-to-one to group peer support, should be smooth and coordinated. This can help to avoid the risk of any withdrawals of support being disorientating or discouraging.
- Communities and families may need to be targeted via awareness raising and education to make sure they are encouraging breastfeeding. Programmes may need to tap into existing social networks to facilitate this.
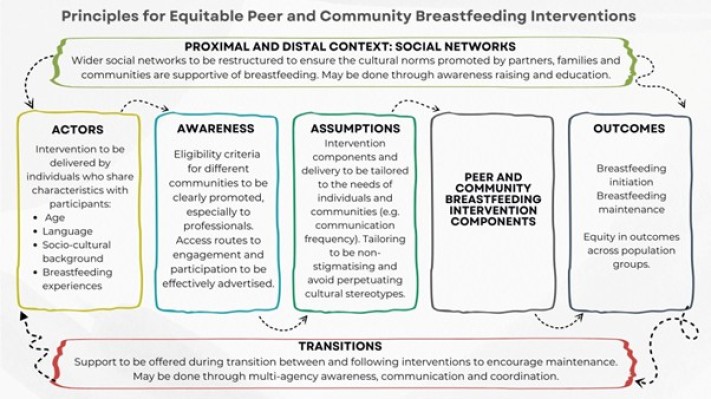
Figure 1. Overview of Principles for Equitable Breastfeeding Programmes
It is important to note that current support approaches delivered through peer and community support programmes do draw on some of these principles, but do not seem to be particularly effective. Programme development needs to be done with the communities at risk of not breastfeeding to make sure that their needs are being fully met.
The role of health visitors
Health visitors can play a vital role to support the realisation of these recommendations:
- Maintaining close links with midwives and maternity services. Health visitors can build upon the breastfeeding advice and care initiated by hospital teams, helping mothers who have started breastfeeding to continue. They can also make sure any feeding issues identified in hospital are followed up.
- Connecting families and resources. Health visitors can ensure mothers and families know about any local drop-in clinics, breastfeeding groups, community cafés, and peer support schemes. They can also coordinate information across these services, ensuring families receive consistent advice and ease transition between them.
- Using their knowledge of the community. Health visitors can help recruit, train, and supervise peer supporters, ensuring the support they deliver is responsive and relevant to the needs of all the women they aim to engage with.
To find out more about the research methods and findings, see our full research briefing.




